
True Costs and Risks of Covid-19 for Immuno-therapy Patients
These days majority of world populations is focused on the statistics and death rate due to Covid-19 infections. Media and news showcase sensational stories and warrant draconian measures to flatten the curve of infection and allow healthcare workers to prepare and treat the patients.
Global flattening of Covid19 infection curve will take toll on cancer medical care
While flattening the curve of Covid19 infections, cancer patients among patients with all other indications need to wait. Not only are they not admitted for screening, but the entire support system, including R&D, early and late stage clinical work needs to be postponed. Most important, their medical care is jeopardized exponentially with health-care system facing overwhelmed delays.
The question is how long can the health system and R&D sustain the suspension without trading the Covid19 lives for other patients/indications:
- clinical trials being suspended or postponed in EU (https://lnkd.in/eqdhHhK ) and China (https://lnkd.in/eZGfr4G)
- hospital service disruptions and non-urgent elective surgeries suspended (https://lnkd.in/ekybkTr )
- research labs closing down and freezing their work (https://lnkd.in/eK4Uy6y )
It may have been necessary to respond in a rapid and non-data-driven manner, which did not require much rationale and strategy. However we had enough time to understand better the viral spread and to know who is the most vulnerable population.
Across different countries the demographical data explain that elderly population ( in particularly > 70 year old) needs to be protected and isolated, while the rest of the population is facing similar risks as with Influenza infection (Iuliano et al., 2018 Lancet; WHO). As of today - March 23rd 2020 - there are 33,276 people infected with SARS-Cov19 in the USA and there were 417 casualties. Germany shows remarkable statistic with 24,873 cases and 94 deaths due to the Covid19 (John Hopkins Resource Center). Even without taking into account that this is very focused testing of patient population, the mortality rate is 1.25% for USA and 0.38% for Germany. Italy with 59,138 infected individuals and 5,476 deaths (i.e. mortality rate 9.26%), which is the cause of global concern and anxiety needs to be explained with additional context. The specifically high excess mortality rate (EMR) in Italy due to Covid19 infection is consistent with significantly higher EMR due to Influenza (eg in seasons from 2013/14 and 2016/17, Rosano et al., 2019 Int J Infect Diseases) and registered among the elderly (average age of victims being 79.5). Further, all of Italy’s victims under 40 have been males with serious existing medical conditions (source Bloomberg, March 18, 2020).

Patients are waiting, diagnosis is being postponed
The ever-changing developments during the last several weeks have surely added to that anxiety of patients who have either recently received an earth-shattering cancer diagnosis and are preparing to undergo the necessary treatments or have been in remission for any amount of time. Not at all helping with this anxiety Cancer Centers (eg. Dana-Farber) have opened discussions as to how to best reduce procedures and tests to try and preserve health care resources. They are encouraging patients to push off ‘routine’ follow up appointments, and stopped performing screening mammograms in asymptomatic patients (Dr. Harold Burstein, a senior physician at Dana-Farber Cancer Institute ).
Each year, 8.8 million people die from cancer. The figure is so high that is accounts for two and a half times more people killed than those who die from HIV/AIDS, tuberculosis and malaria combined.
In 2018, there were more than 18 million new cases of cancer diagnosed, of which nearly 5 million cases of breast, cervical, colorectal, and oral cancers could have been detected sooner and treated more effectively.
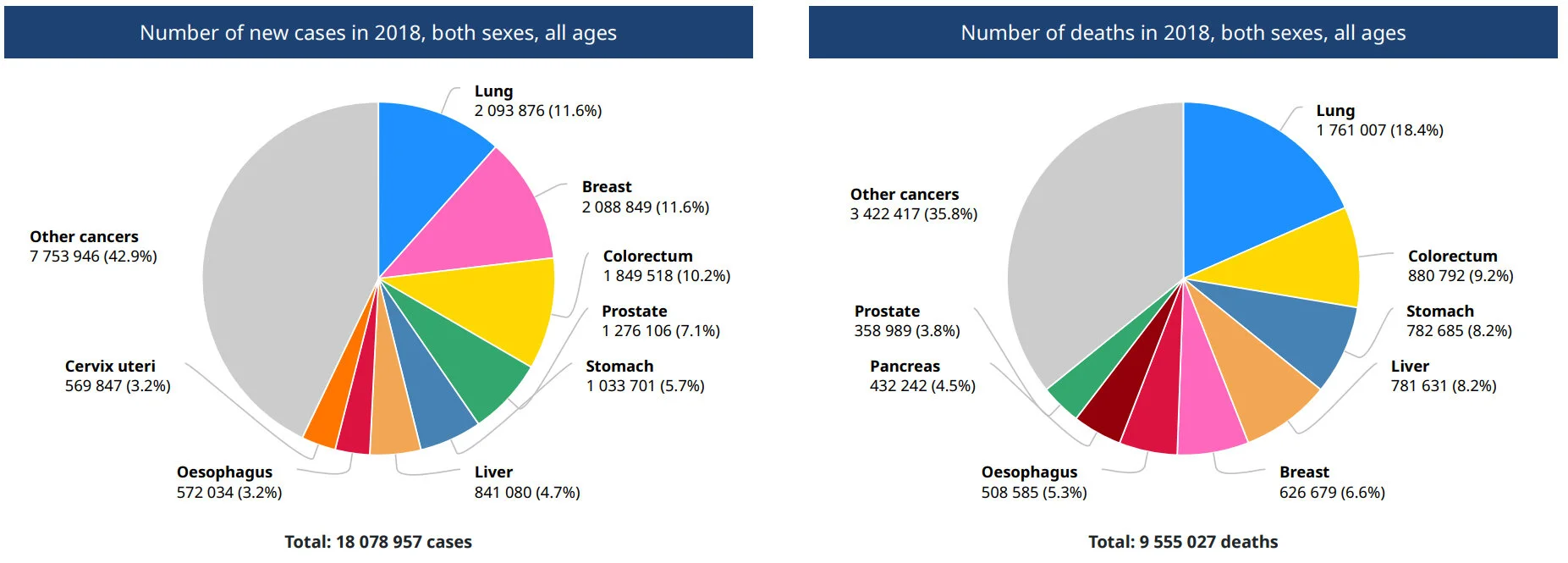
Cancer incidence and mortality statistics worldwide. (WHO)
In the United States, the 5-year survival rate for women diagnosed with cervical cancer at an advanced stage is 15%, compared to 93% if diagnosed when the cancer has not spread. Colon cancer caught early has a 91% 5-year survival rate, vs. an only 11% survival rate if it is caught late and has spread to other organs. Among the 15% of ovarian cancer cases diagnosed early when cancer is confined to the ovary, over 90% survive five years. Unfortunately, for the nearly two-thirds diagnosed after it has spread, only 28% survive that long. Early detection is also key in breast and prostate cancers. Five-year survival for breast- and prostate-cancer patients with early stage disease is 98% and 100%, respectively, and survival rates remain high at 10 years.

Chances of survival are greater if cancer is diagnosed when still confined to the organ of origin (stage I). Survival rates decline as tumors enlarge and spread regionally (stages II,III) or distantly (stage IV). (Canary Foundation)
Achieving earlier diagnosis for non-small cell lung cancer alone would generate an additional 4,275 years of life for lung cancer in UK alone.

Calculation of additional years of life gained by achieving the stage distribution of the best CCG in England (Cancer Research UK, 2014)
If this is not convincing enough, early stage cancer treatment is significantly less expensive than treatment for advanced disease. Taking together for cancer types (colon, rectal, ovarian and lung), achieving the level of early diagnosis comparable with the best in England could deliver savings of over £44 million, benefiting nearly 11,100 patients. Due to the higher level of recurrence that occurs in lung cancer, achieving this level of earlier diagnosis would incur a cost of £6.4 millions (Cancer Research UK, 2014).
The Impact of CAR T-Cell Treatment Delays on Society
The magnitude of CAR T-cell therapy’s value depends on timely patient access. Given the aggressive nature of relapsed/refractory disease, patients eligible for CAR T may have to settle for less efficacious third- or fourth-line therapies or even die while waiting for CAR T therapy.
Recent study by Snider et al., 2019 measured the social value of CAR T-cell therapy (CAR T) for relapsed or refractory pediatric acute lymphoblastic leukemia (pALL) and diffuse large B-cell lymphoma in the United States and quantified social value lost due to treatment delays. They used an economic framework for therapy valuation, measuring social value as the sum of consumer surplus and manufacturer profit. Consumer surplus is the difference between the value of health gains from a therapy and its incremental cost, while accounting for indirect costs and benefits to patients. Social value analyses can complement cost-effectiveness analyses by shedding light on the access/innovation trade-off.
When treatment is delayed, social value is lost for both patients and manufacturers: Patients lose access to health gains from the treatment, and manufacturer profit is reduced. Depending on production costs, as much as $6.5 billion and $34.8 billion in social value was generated for patients with pALL and DLBCL, respectively. However, with 1, 2, or 6 months of treatment delay (assuming $200,000 production costs), the pALL population lost 9.8%, 36.2%, and 67.3% of social value, respectively, whereas the DLBCL population lost 4.2%, 11.5%, and 46.0%, relative to no delay.

QUALYs and productivity lost per patient for treatment delays for CART cell therapies for patients with pALL and DLBCL in the first treatment cohort, relative to no delay. (Snider et al., 2019)
Covid19 thread to laboratory research and early clinical trials
With the effects of the Covid19 reaching every corner of the health care field, clinical trials for the development of life-saving cancer drugs have seen an enormous impact.
Immune checkpoint inhibitors (ICI) can improve overall survival for patients with advanced cancers such as melanoma and non-small-cell lung cancer (Conforti et al, 2018, Lancet). However, despite an incredible progress in the decade of cancer immunotherapy (reviewed by Arthur N. Brodsky, Ph.D.), more work remains to be done because many cancer patients still don’t respond to immunotherapy. While much of the “low-hanging fruit” of immunotherapy has already been plucked for the benefit of patients, the solutions to the field’s remaining challenges will require even more intense investigation and collaboration. (Dr. Sharma: Cancer Immunotherapy: 2020 Research Update and a Look Ahead).
Hundreds of new and promising cancer immunotherapy treatments are only available to patients in clinical trials. Participating in clinical trials of these therapies may be the most promising option for cancer patients today, and will be critical to speeding the development and approval of new drugs for more patients in the future.
The two main treatment modalities are checkpoint inhibitors (CPIs) and chimeric antigen receptor (CAR) T cells. Regarding the regional distribution of registered clinical immunotherapy trials a shift from PD-1 / PD-L1 trials (mainly performed in the US and Europe) to CAR T cell trials (majority of trials performed in the US and China) can be noted. For checkpoint blockade, current studies focus on combinational approaches, perioperative use, new tumor entities, response prediction, toxicity management and use in special patient populations. Regarding cellular immunotherapy, recent studies confirmed safety and efficacy of CAR T cells in larger cohorts of patients with acute lymphoblastic leukemia or diffuse large B cell lymphoma. Different strategies to translate the striking success of CAR T cells in B cell malignancies to other hematological and solid cancer types are currently under clinical investigation.
While there aren’t any treatment trials that have taken a pause, there is a postponement in the opening of new trials or the enrollment of new patients on trials. Besides, patients stopped coming into the clinics among others due to local rules that may govern travel, or been told to stay home, causing severe disruptions for ongoing clinical trials.
Further, research in hundreds of labs across the globe, on everything from Alzheimer's to cancer, is stalled and the labs have been put into hibernation. The decisions have been implemented at Harvard, Stanford, Duke and Rice universities, the Massachusetts Institute of Technology, and elsewhere. In some cases the decision was to keep some long-running experiments going, monitored by a skeleton crew, freeze some other cells to hopefully thaw out later, and the rest of the experiments went into the garbage. While the research on the coronavirus will continue, as for non-coronavirus research - with the neccessary precautions -it will likely slow the pace and be really disruptive . The question is for how long it is possible to mitigate and ensure the damage to the research enterprise will not ensue in major casualties of the patients.
We need to re-think our strategy of drastic shut down and implement a thought-through approach introducing restrictions targeting specifically vulnerable population
As our society faces an illness as Covid19 that is serious and devastating, we need to continue help unmet-medical need patients. Next wave(s) indicate we are facing indefinite period of Covid19 (https://lnkd.in/eDyrSg6). We are too interconnected for effective global isolation and it would be naive to believe social distancing and isolation, which can only be limited to its extent and time, won’t ensue in unprecedented harm for the society. We need to re-allocate the resources from communities with sufficient capacities to areas where medical care is collapsing, but ensuring long-term benefit for current and prospective patients.
When we are busy trying to survive individually and as a society, let's not forget the indications which need our dedication and focus for effective medical care today and in the long term.
As the R&D community we need to urge the governments to revisit the measures and take into account global patient population, including cancer patients which in most cases do not have time. Currently we are not part of the solution, we are part of the crisis.



